 The Independent Uganda: You get the Truth we Pay the Price
The Independent Uganda: You get the Truth we Pay the Price



How Uganda’s group support psychotherapy is reshaping mental‑health care for people living with HIV
ANALYSIS | PATRICIA AKANKWATSA | When Dr Etheldreda Nakimuli-Mpungu speaks about depression and HIV, she does so with the measured tone of a researcher — but also with the urgency of someone who has witnessed the quiet suffering behind the statistics.
Across sub-Saharan Africa, millions of people are living longer because of antiretroviral therapy (ART). Clinics that once focused on emergency treatment now manage HIV as a chronic condition. Viral suppression rates have improved. Deaths have fallen. In many communities, HIV is no longer the near-certain death sentence it once was.
Yet, beneath these gains lies a less visible crisis.
“Mental health problems drive enormous suffering, especially in low- and middle-income countries where access to care is lowest,” Dr Nakimuli-Mpungu told delegates during a recent webinar organised by the International AIDS Society. The event examined the intersection of HIV and non-communicable diseases — an area gaining increasing attention among global health experts.
One statistic in particular stood out. “One in three people on antiretroviral therapy in Africa experience significant depressive symptoms,” she said. “These interfere with adherence and reduce viral suppression. Group support psychotherapy offers hope.”
A barrier hidden in plain sight
The figure — roughly one in three — is consistent with multiple systematic reviews estimating that between 25% and 35% of people living with HIV in sub-Saharan Africa experience clinically significant depressive symptoms.
Depression is not simply a co-existing condition. Research consistently shows it directly undermines HIV treatment outcomes. People experiencing depression are less likely to take medication consistently, less likely to attend follow-up appointments and less likely to achieve viral suppression. Over time, this increases the risk of illness, transmission and death.
In other words, untreated depression disrupts the entire HIV care cascade.
For years, mental health was treated as secondary — an optional add-on in already stretched health systems. HIV programmes were built around laboratory monitoring, drug procurement and viral load suppression targets. Psychosocial care often remained underfunded and under-prioritised.
Dr Nakimuli and her colleagues argue that this separation is no longer tenable.
A community-based response
In response to these realities, her team developed Group Support Psychotherapy (GSP) — an eight-session, gender-specific programme delivered within communities.
Rather than relying on specialist psychiatrists — who are scarce in many African countries — the intervention is facilitated by trained community members of the same gender as participants. The sessions combine mental health education, emotional processing, coping strategies, stigma reduction and livelihood training.
The design reflects a deeper understanding of depression among people living with HIV. It is rarely driven by biology alone. Poverty, unemployment, stigma, isolation and economic insecurity all intersect to produce psychological distress.
By blending cognitive-behavioural techniques with elements of social support and sustainable livelihoods training, the programme attempts to address both emotional and economic vulnerability.
“It’s not enough to tell someone to think positively,” Dr Nakimuli-Mpungu explained. “If they have no income, face stigma and feel isolated, those realities must also be addressed.”
Testing the model
The intervention was subjected to rigorous scientific evaluation through a randomised controlled trial — the gold standard in clinical research.
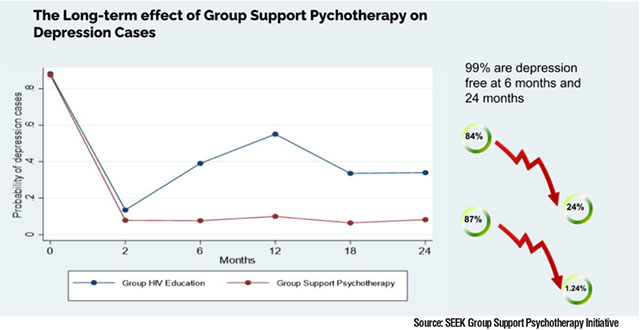
Participants who received Group Support Psychotherapy showed significant reductions in depressive symptoms compared with those who did not. Importantly, improvements were not limited to mental health. ART adherence improved, and rates of viral suppression increased.
The findings challenged a long-standing assumption: that psychosocial interventions are too expensive or too complex to scale in low-resource settings.
But the research did not stop at measuring whether the programme worked. The team sought to understand how it worked — and for whom.
Using advanced analytical approaches, including predictive modelling and causal mediation analysis, they examined the pathways that led to recovery.
The results offered practical insights for policymakers and programme designers.
Who benefits — and why
The strongest predictor of recovery was simple: being assigned to the therapy group. That confirmed the intervention’s effectiveness.
However, additional patterns emerged. People who began the programme with low levels of perceived social support were less likely to recover fully. Socioeconomic vulnerability — low income, minimal savings and limited assets — also predicted poorer outcomes. High baseline stigma, prolonged unemployment and older age were additional risk factors.
Conversely, individuals who started with higher levels of self-esteem tended to respond more positively.
The mediation analysis provided further clarity. Of the psychosocial mechanisms measured, increased emotional support-seeking during therapy emerged as the key driver of early recovery. Participants who learned to reach out for emotional support — from peers, family or community members — experienced faster improvements.
Over time, reductions in stigma and improvements in income-generating activity became critical in sustaining recovery. By 12 months, participants showed measurable gains in livelihood indicators. Decreased stigma was closely linked to increased economic participation.
“Emotional support-seeking drives early recovery, while stigma reduction and livelihood gains sustain it,” Dr Nakimuli-Mpungu said. “These findings show not only that community solutions can be effective, but how they work.”
A funding crossroads
The case for integration comes at a delicate moment. Yves Miel Zuñiga of United for Global Mental Health, speaking at the same webinar, warned that funding contractions are already affecting access to care.
“Communities are not waiting. They’re already building integrated solutions,” he said, pointing to grassroots advocacy, peer support networks and community health workers bridging service gaps.
But he highlighted a stark reality: “We found that 750,000 people immediately lost mental health care at the time of the cuts.”
For advocates, the message is clear — demand exists, communities are mobilised, but formal financing and health systems must catch up.
Policy shifts at the global level
International guidance is beginning to reflect this shift. In 2025, the World Health Organization updated its recommendations on integrating mental health, diabetes and hypertension services within HIV programmes. The revisions strengthened previous guidance, signalling that mental health integration is no longer optional.
Helen Bygrave, from the International AIDS Society’s Differentiated Service Delivery programme, summarised the evidence underpinning the changes. Systematic reviews commissioned for the WHO updates found that integrating mental health services into HIV care improves retention and viral suppression while significantly reducing depression severity.
She pointed to a multi-country cluster-randomised trial across East Africa comparing disease-specific “vertical” clinics with a one-stop chronic-care model. Preliminary findings suggested that integration maintained viral suppression, improved management of other chronic conditions and, importantly for constrained budgets, demonstrated cost efficiencies for both health systems and patients.
Despite encouraging policy signals, implementation gaps remain substantial. Frontline health workers in Uganda and Kenya report that training often focuses on diagnosing depression rather than providing practical counselling skills. Many clinicians say they are taught to identify symptoms but not how to sit with a patient in distress or offer structured psychosocial support.
Mental health is frequently absent from routine supervision and national programme planning. Under pressure from competing priorities, decision-makers may relegate psychosocial care until crises emerge.
Financing patterns reinforce this imbalance. Reviews of Global Fund and national investment plans show mental health increasingly mentioned in policy narratives, but dedicated funding lines remain limited. Analysts describe a gap between rhetoric and resources.
The case for person-centred care
Experts increasingly advocate for person-centred, differentiated service delivery models.
Such approaches align medication refill schedules, decentralise care to community distribution points and clarify which health workers can screen and manage multiple chronic conditions.
Several countries are piloting integrated chronic-care models that combine HIV services with hypertension and diabetes management. Early cost-effectiveness signals are encouraging — a crucial consideration as governments and donors recalibrate sustainability plans.
For implementers, the lessons are pragmatic.
First, invest in scalable, community-based psychosocial interventions delivered by non-specialists.
Second, use predictive tools to identify those at highest risk of persistent depression and design stepped-care pathways offering additional economic or social support.
Third, protect funding for community system strengthening so that integration becomes operational reality rather than policy aspiration.
Lives behind the data
For participants in Group Support Psychotherapy sessions across Ugandan communities, the impact has been tangible.
Faster emotional recovery. Reduced stigma. New coping strategies. Improved income-generating activity.
These changes, taken together, make adherence to HIV treatment more achievable — and viral suppression more sustainable.
In global health, progress is often measured in percentages and prevalence rates. But behind each statistic is a person navigating illness, poverty and stigma.
The science now suggests that treating HIV effectively may depend as much on addressing emotional and social realities as on delivering medication.
“If communities heal faster together,” Dr Nakimuli-Mpungu said, “we must give them the tools and the budget to do so.”
As African countries move into a new phase of chronic disease management, the challenge is clear: ensure that the next chapter of the HIV response recognises that mental health is not peripheral to care — it is central to it.


